


 Sign Out
Sign Out

However, the efficacy of aripiprazole may be mediated through a combination of partial agonist activity at D2 and 5-HT1A receptors and antagonist activity at 5-HT2A receptors. Actions at receptors other than D2, 5-HT1A, and 5-HT2A may explain some of the other adverse reactions of aripiprazole (e.g., the orthostatic hypotension observed with aripiprazole may be explained by its antagonist activity at adrenergic alpha1 receptors).
Pharmacodynamics: Aripiprazole exhibits high affinity for dopamine D2 and D3, serotonin 5-HT1A and 5-HT2A receptors (Ki values of 0.34 nM, 0.8 nM, 1.7 nM, and 3.4 nM, respectively), moderate affinity for dopamine D4, serotonin 5-HT2C and 5-HT7, alpha1-adrenergic and histamine H1 receptors (Ki values of 44 nM, 15 nM, 39 nM, 57 nM, and 61 nM, respectively), and moderate affinity for the serotonin reuptake site (Ki=98 nM). Aripiprazole has no appreciable affinity for cholinergic muscarinic receptors (IC50>1000 nM). Aripiprazole functions as a partial agonist at the dopamine D2 and the serotonin 5-HT1A receptors, and as an antagonist at serotonin 5-HT2A receptor.
Alcohol: There was no significant difference between oral aripiprazole co-administered with ethanol and placebo co-administered with ethanol on performance of gross motor skills or stimulus response in healthy subjects. As with most psychoactive medications, patients should be advised to avoid alcohol while taking ABILIFY MAINTENA.
CLINICAL STUDIES: Schizophrenia: The efficacy of ABILIFY MAINTENA for treatment of schizophrenia was established in: One short-term (12-week), randomized, double-blind, placebo-controlled trial in acutely relapsed adults, Protocol 31-12-291 (Study 1); One longer-term, double-blind, placebo-controlled, randomized-withdrawal (maintenance) trial in adults, Protocol 31-07-246 (Study 2).
Short-Term Efficacy: In the short-term (12-week), randomized, double-blind, placebo-controlled trial in acutely relapsed adults (Study 1), the primary measure used for assessing psychiatric signs and symptoms was the Positive and Negative Syndrome Scale (PANSS). The PANSS is a 30 item scale that measures positive symptoms of schizophrenia (7 items), negative symptoms of schizophrenia (7 items), and general psychopathology (16 items), each rated on a scale of 1 (absent) to 7 (extreme); total PANSS scores range from 30 to 210. The primary endpoint was the change from baseline in PANSS total score to week 10.
The inclusion criteria for this short-term trial included adult inpatients who met DSM-IV-TR criteria for schizophrenia. In addition, all patients entering the trial must have experienced an acute psychotic episode as defined by both PANSS Total Score ≥ 80 and a PANSS score of > 4 on each of four specific psychotic symptoms (conceptual disorganization, hallucinatory behavior, suspiciousness/persecution, unusual thought content) at screening and baseline. The key secondary endpoint was the change from baseline in Clinical Global Impression-Severity (CGI-S) assessment scale to week 10. The CGI-S rates the severity of mental illness on a scale of 1 (normal) to 7 (among the most extremely ill) based on the total clinical experience of the rater in treating patients with schizophrenia. Patients had a mean PANSS total score of 103 (range 82 to 144) and a CGI-S score of 5.2 (markedly ill) at entry.
In this 12-week study (n=339) comparing ABILIFY MAINTENA (n=167) to placebo (n=172), patients were administered 400 mg ABILIFY MAINTENA or placebo on days 0, 28, and 56. The dose could be adjusted down and up within the range of 400 to 300 mg on a one time basis. ABILIFY MAINTENA was superior to placebo in improving the PANSS total score at the end of week 10 (see Table 1).
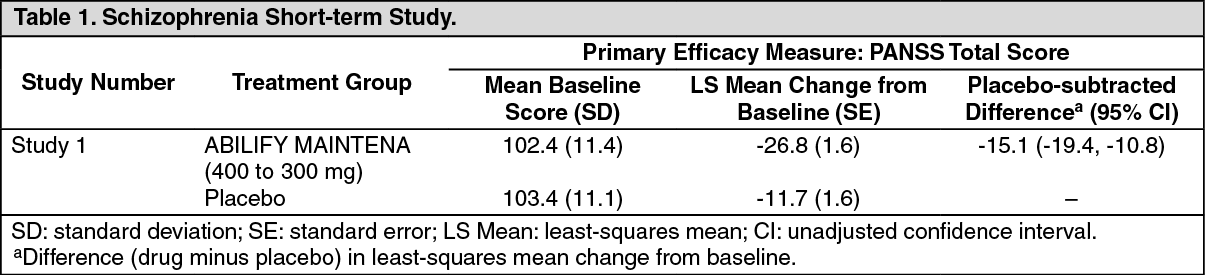 Click on icon to see table/diagram/image
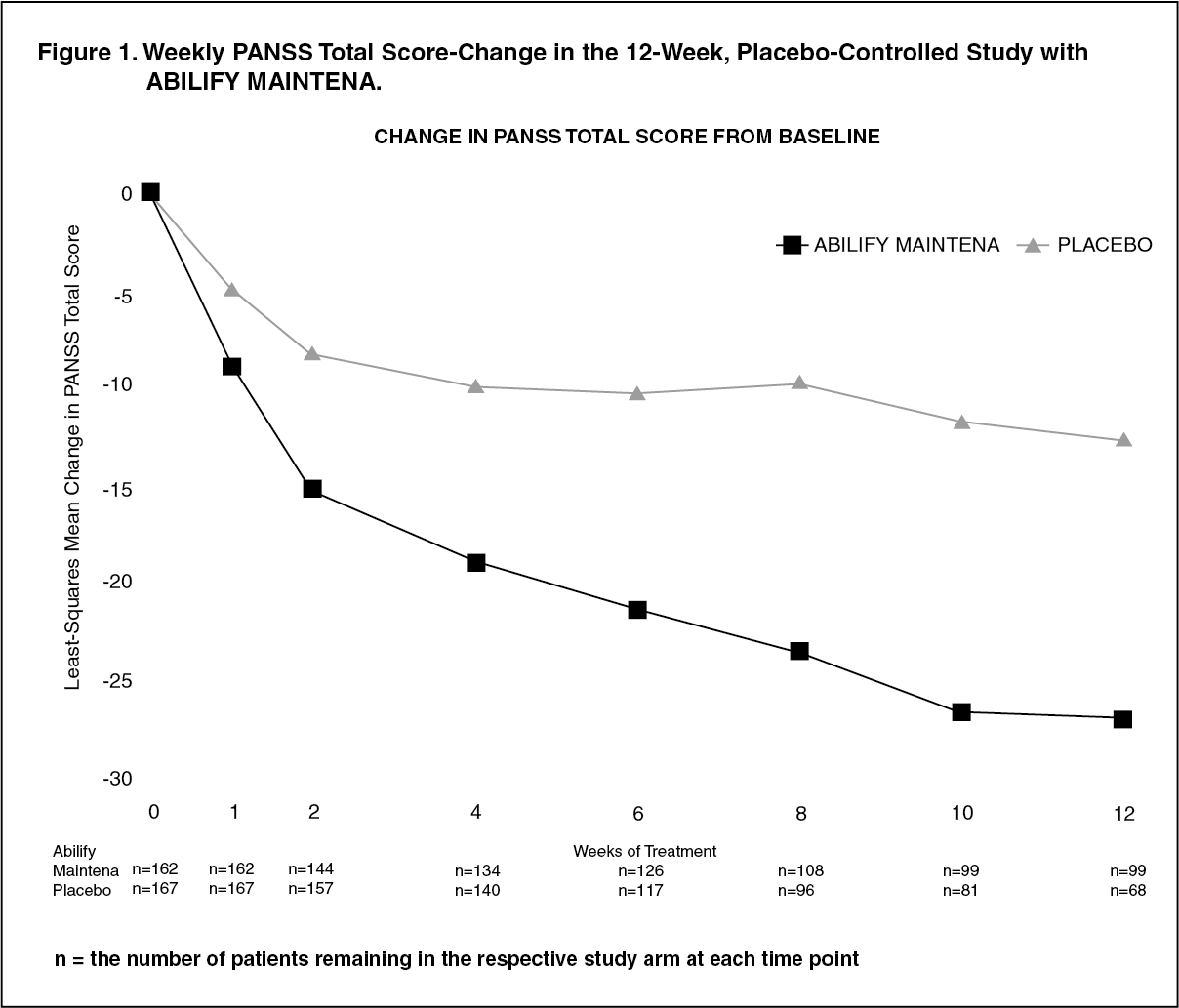
Click on icon to see table/diagram/imageThe change in PANSS total score by week is shown in Figure 1. ABILIFY MAINTENA also showed improvement in symptoms represented by CGI-S score mean change from baseline to week 10. The results of exploratory subgroup analyses by gender, race, age, ethnicity, and BMI were similar to the results of the overall population. (See Figure 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageLonger-Term Efficacy: The efficacy of ABILIFY MAINTENA in maintaining symptomatic control in schizophrenia was established in a double-blind, placebo-controlled, randomized-withdrawal trial in adult patients (Study 2) who met DSM-IV-TR criteria for schizophrenia and who were being treated with at least one antipsychotic medication. Patients had at least a 3-year history of illness and a history of relapse or symptom exacerbation when not receiving antipsychotic treatment.
In addition to the PANSS and CGI-S, clinical ratings during this trial included the: Clinical Global Impression-Improvement (CGI-I) scale, a scale of 1 (very much improved) to 7 (very much worse) based on the change from baseline in clinical condition and Clinical Global Impression-Severity of Suicide (CGI-SS) scale, which is comprised of 2 parts: Part 1 rates the severity of suicidal thoughts and behavior on a scale of 1 (not at all suicidal) to 5 (attempted suicide) based on the most severe level in the last 7 days from all information available to the rater and Part 2 rates the change from baseline in suicidal thoughts and behavior on a scale of 1 (very much improved) to 7 (very much worse).
This trial included: A 4 to 6 week open-label, oral conversion phase for patients on antipsychotic medications other than aripiprazole. A total of 633 patients entered this phase.
An open-label, oral aripiprazole stabilization phase (target dose of 10 mg to 30 mg once daily). A total of 710 patients entered this phase. Patients were 18 to 60 years old (mean 40 years) and 60% were male. The mean PANSS total score was 66 (range 33 to 124). The mean CGI-S score was 3.5 (mildly to moderately ill). Prior to the next phase, stabilization was required. Stabilization was defined as having all of the following for four consecutive weeks: an outpatient status, PANSS total score ≤80, CGI-S ≤4 (moderately ill), and CGI-SS score ≤2 (mildly suicidal) on Part 1 and ≤5 (minimally worsened) on Part 2; and a score of ≤4 on each of the following PANSS items: conceptual disorganization, suspiciousness, hallucinatory behavior, and unusual thought content.
A minimum 12-week uncontrolled, single-blind ABILIFY MAINTENA stabilization phase (treatment with 400 mg of ABILIFY MAINTENA given every 4 weeks in conjunction with oral aripiprazole [10 mg to 20 mg/day] for the first 2 weeks). The dose of ABILIFY MAINTENA may have been decreased to 300 mg due to adverse reactions. A total of 576 patients entered this phase. The mean PANSS total score was 59 (range 30 to 80) and the mean CGI-S score was 3.2 (mildly ill). Prior to the next phase, stabilization was required (see previous text for the definition of stabilization) for 12 consecutive weeks.
A double-blind, placebo-controlled randomized-withdrawal phase to observe for relapse (defined as follows). A total of 403 patients were randomized 2:1 to the same dose of ABILIFY MAINTENA they were receiving at the end of the stabilization phase, (400 mg or 300 mg administered once every 4 weeks) or placebo. Patients had a mean PANSS total score of 55 (range 31 to 80) and a CGI-S score of 2.9 (mildly ill) at entry. The dose could be adjusted up and down or down and up within the range of 300 to 400 mg on a one time basis.
The primary efficacy endpoint was time from randomization to relapse. Relapse was defined as the first occurrence of one or more of the following criteria: CGI-I of ≥5 (minimally worse) and an increase on any of the following individual PANSS items (conceptual disorganization, hallucinatory behavior, suspiciousness, unusual thought content) to a score >4 with an absolute increase of ≥2 on that specific item since randomization or an increase on any of the following individual PANSS items (conceptual disorganization, hallucinatory behavior, suspiciousness, unusual thought content) to a score >4 and an absolute increase ≥4 on the combined four PANSS items (conceptual disorganization, hallucinatory behavior, suspiciousness, unusual thought content) since randomization; Hospitalization due to worsening of psychotic symptoms (including partial hospitalization), but excluding hospitalization for psychosocial reasons; CGI-SS of 4 (severely suicidal) or 5 (attempted suicide) on Part 1 and/or 6 (much worse) or 7 (very much worse) on Part 2; or Violent behavior resulting in clinically significant self-injury, injury to another person, or property damage.
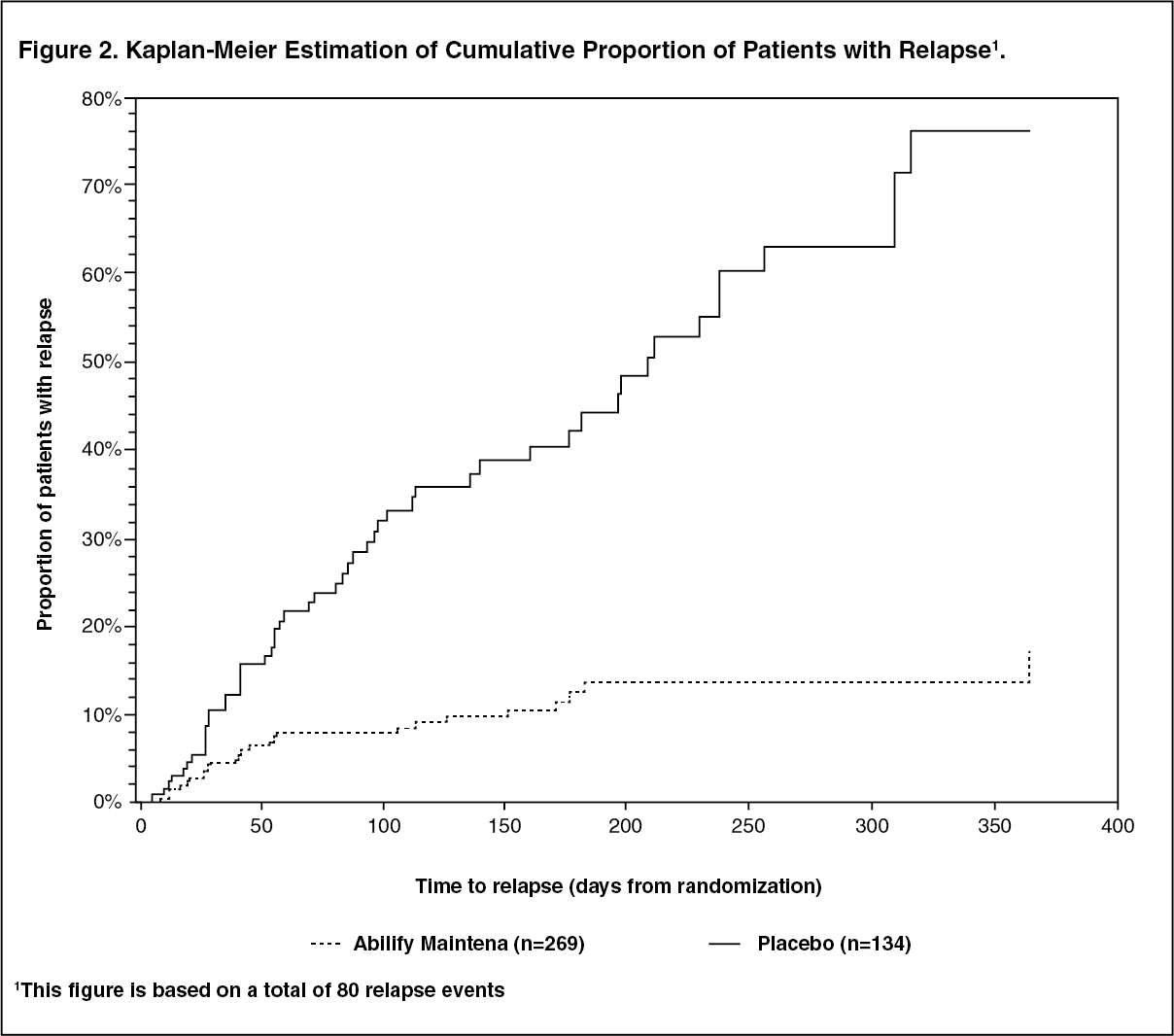
A pre-planned interim analysis demonstrated a statistically significantly longer time to relapse in patients randomized to the ABILIFY MAINTENA group compared to placebo-treated patients and the trial was subsequently terminated early because maintenance of efficacy was demonstrated. The final analysis demonstrated a statistically significantly longer time to relapse in patients randomized to the ABILIFY MAINTENA group than compared to placebo-treated patients. The Kaplan-Meier curves of the cumulative proportion of patients with relapse during the double-blind treatment phase for ABILIFY MAINTENA and placebo groups are shown in Figure 2. (See Figure 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe key secondary efficacy endpoint, percentage of subjects meeting the relapse criteria, was statistically significantly lower in patients randomized to the ABILIFY MAINTENA group (10%) than in the placebo group (40%).
Bipolar I Disorder - Maintenance Monotherapy: The efficacy of ABILIFY MAINTENA for the maintenance treatment of bipolar I disorder was established in a 52-week double-blind, placebo-controlled, randomized withdrawal trial in adult patients who were experiencing a manic episode at trial entry, met DSM-IV-TR criteria for bipolar I disorder, and had a history of at least one previous manic or mixed episode with manic symptoms of sufficient severity to require one of the following interventions: hospitalization and/or treatment with a mood stabilizer, and/or treatment with an antipsychotic agent.
Clinical ratings during this trial included: Young Mania Rating Scale (YMRS): an 11-item, clinician-rated scale used to assess the degree of manic symptomatology, in a range with 0 representing no symptoms, and 60 representing worst symptoms.
Montgomery-Asberg Depression Rating Scale (MADRS): a 10-item clinician-related scale used to assess the degree of depressive symptomatology, with 1 representing no symptoms, and 60 representing worst symptoms.
Clinical Global Impression Bipolar Version Severity of Illness (CGI-BP-S): a scale of 1 (normal, not at all ill) to 7 (very severely ill patient) based on the patient's severity of illness mania, depression, and overall bipolar illness.
This trial included: A 4 to 6 week, open-label, oral conversion phase for patients on treatments for bipolar I disorder other than aripiprazole. A total of 466 patients entered this phase.
A 2 to 8 week, open-label, oral aripiprazole stabilization phase (target dose of 15 mg to 30 mg once daily). A total of 632 patients entered this phase. Patients were 18 to 65 years old (mean 40.7 years) and 60% were female. The mean (range) baseline scores were: YMRS total, 16.9 MADRS total, 5.7, and CGI-BP-S overall, 3.4 (mildly to moderately ill). Prior to the next phase, stabilization was required. Stabilization was defined as having all of the following at one bi-weekly visit: Outpatient status, YMRS total score ≤12, MADRS total score ≤12, no active suicidality; with active suicidality defined as a score of 4 or more on the MADRS item 10 OR an answer of "yes" on question 4 or 5 on the Columbia Suicide Severity Rating Scale (C-SSRS).
A minimum 12-week, uncontrolled, single-blind ABILIFY MAINTENA stabilization phase (treatment with 400 mg of ABILIFY MAINTENA given every 4 weeks in conjunction with oral aripiprazole [10 mg to 20 mg/day] for the first 2 weeks). The dose of ABILIFY MAINTENA was allowed to be decreased to 300 mg due to adverse reactions. A total of 425 patients entered this phase. The mean (range) baseline scores were: YMRS total, 5.8, MADRS total 3.7, and CGI-BP-S overall, 2.1 (minimally ill). Prior to the next phase, stabilization was required (see previous text for the definition of stabilization) for 8 consecutive weeks starting at week 6.
A double-blind, placebo-controlled, randomized-withdrawal phase to observe for recurrence to a mood episode (defined as follows) for up to 52 weeks. A total of 266 patients were randomized 1:1 to the same dose of ABILIFY MAINTENA they were receiving at the end of the stabilization phase, (400 mg or 300 mg administered once every 4 weeks) or placebo. The mean (range) baseline scores were: YMRS total, 2.8 (0 to 12), MADRS total, 2.7 (0 to 12), and CGI-S overall, 1.7 (minimally ill). The dose could be decreased to 300 mg for tolerability and returned once to 400 mg.
The primary efficacy endpoint was time from randomization to recurrence of any mood episode. Recurrence was defined as the first occurrence of one or more of the following criteria: Hospitalization for any mood episode OR Any of the following: YMRS total score ≥15 OR MADRS total score ≥15 OR Clinical Global Impression - Bipolar Version-Severity (CGI-BP-S) score >4 (overall score) OR Serious adverse event (SAE) of worsening disease (bipolar I disorder) OR Discontinuation due to lack of efficacy or discontinuation due to an adverse event (AE) of worsening disease OR Clinical worsening with the need for addition of a mood stabilizer, antidepressant treatment, antipsychotic medication, and/or increase greater than the allowed benzodiazepine doses for treatment of symptoms of an underlying mood disorder OR Active suicidality, which is defined as a score of 4 or more on the MADRS item 10 OR an answer of "yes" on question 4 or 5 on the C-SSRS.
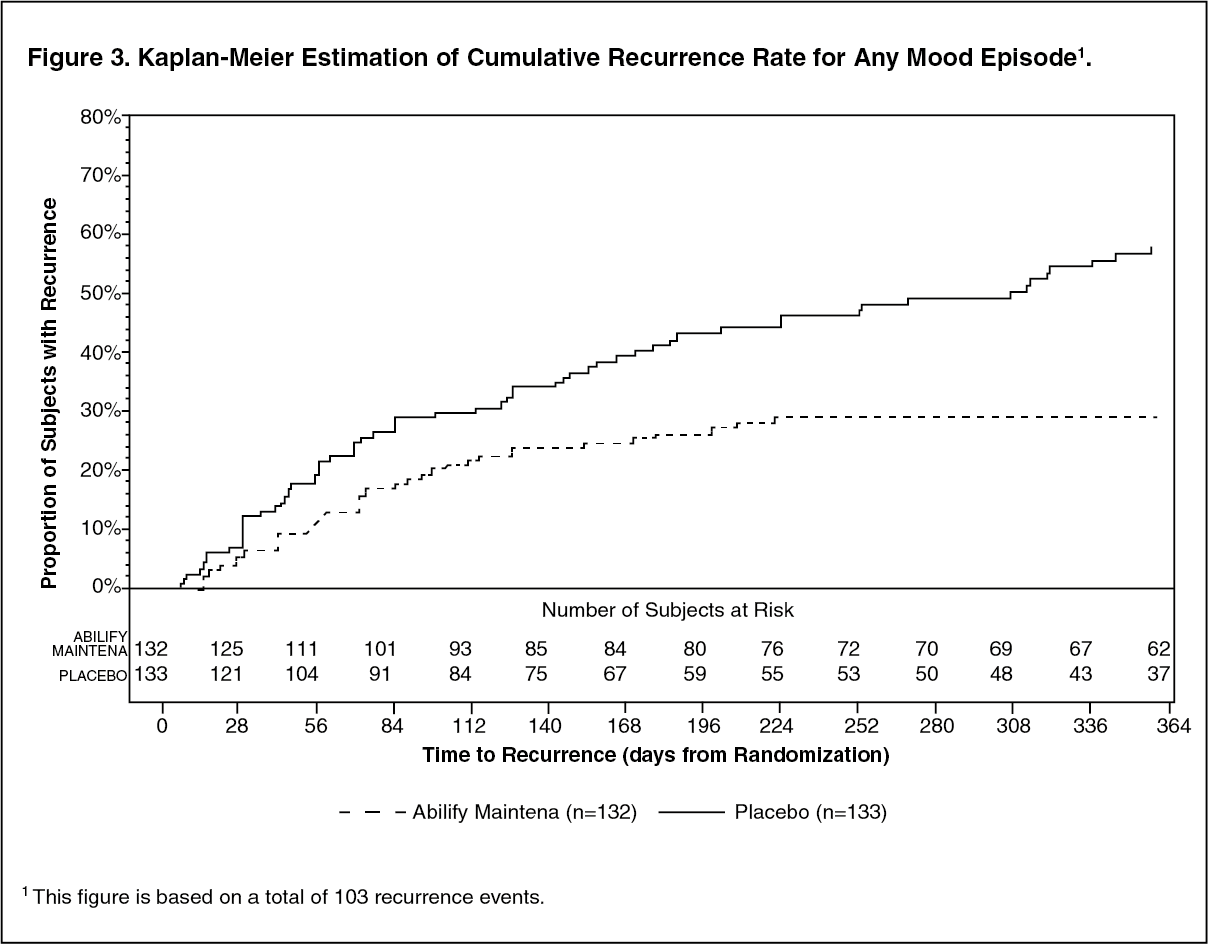
Analysis demonstrated a statistically significantly longer time to recurrence of any mood episode in subjects randomized to the ABILIFY MAINTENA group than compared to placebo-treated subjects. The Kaplan-Meier curves of the time of recurrence to any mood episode during the double-blind treatment phase for ABILIFY MAINTENA and placebo groups are shown in Figure 3. (See Figure 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAnalysis by type of mood recurrence demonstrated a statistically significantly longer time to recurrence for both manic and mixed mood episodes in subjects treated with ABILIFY MAINTENA compared to those treated with placebo. There was no substantial difference between treatment groups in delaying time to recurrence of depressive mood episodes.
An examination of subgroups did not reveal any clear evidence of differential responsiveness on the basis of age, sex, or race.
Pharmacokinetics: ABILIFY MAINTENA activity is presumably primarily due to the parent drug, aripiprazole, and to a lesser extent, to its major metabolite, dehydro-aripiprazole, which has been shown to have affinities for D2 receptors similar to the parent drug and represents about 29% of the parent drug exposure in plasma.
Aripiprazole absorption into the systemic circulation is slow and prolonged following intramuscular injection due to low solubility of aripiprazole particles. Following a single dose administration of ABILIFY MAINTENA in the deltoid and gluteal muscle, the extent of absorption (AUCt, AUC∞) of aripiprazole was similar for both injection sites, but the rate of absorption (Cmax) was 31% higher following administration to the deltoid compared to the gluteal site. However, at steady state, AUC and Cmax were similar for both sites of injection. Following multiple intramuscular doses, the plasma concentrations of aripiprazole gradually rise to maximum plasma concentrations at a median Tmax of 5 - 7 days for the gluteal muscle and 4 days for the deltoid muscle. After gluteal administration, the mean apparent aripiprazole terminal elimination half-life was 29.9 days and 46.5 days after multiple injections for every 4-week injection of ABILIFY MAINTENA 300 mg and 400 mg, respectively. Steady state concentrations for the typical subject were attained by the fourth dose for both sites of administration. Approximate dose-proportional increases in aripiprazole and dehydro-aripiprazole exposure were observed after every four week ABILIFY MAINTENA injections of 300 mg and 400 mg.
Elimination of aripiprazole is mainly through hepatic metabolism involving two P450 isozymes, CYP2D6 and CYP3A4. Aripiprazole is not a substrate of CYP1A1, CYP1A2, CYP2A6, CYP2B6, CYP2C8, CYP2C9, CYP2C19, or CYP2E1 enzymes. Aripiprazole also does not undergo direct glucuronidation.
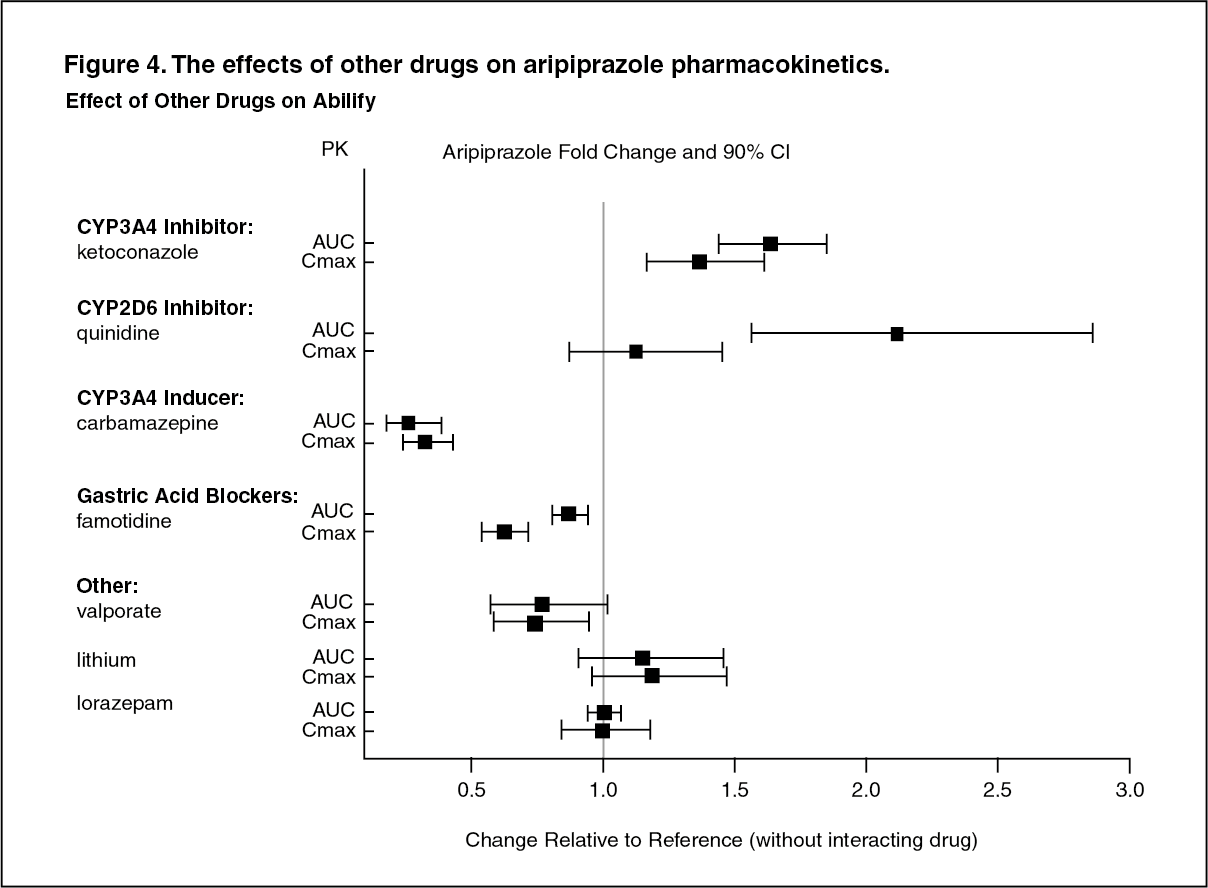
Drug Interaction Studies: No specific drug interaction studies have been performed with ABILIFY MAINTENA. The information as follows is obtained from studies with oral aripiprazole.
Effects of other drugs on the exposures of aripiprazole and dehydro-aripiprazole are summarized in Figure 4 and Figure 5, respectively. Based on simulation, a 4.5-fold increase in mean Cmax and AUC values at steady-state is expected when extensive metabolizers of CYP2D6 are administered with both strong CYP2D6 and CYP3A4 inhibitors. After oral administration, a 3-fold increase in mean Cmax and AUC values at steady-state is expected in poor metabolizers of CYP2D6 administered with strong CYP3A4 inhibitors. (See Figures 4 and 5.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image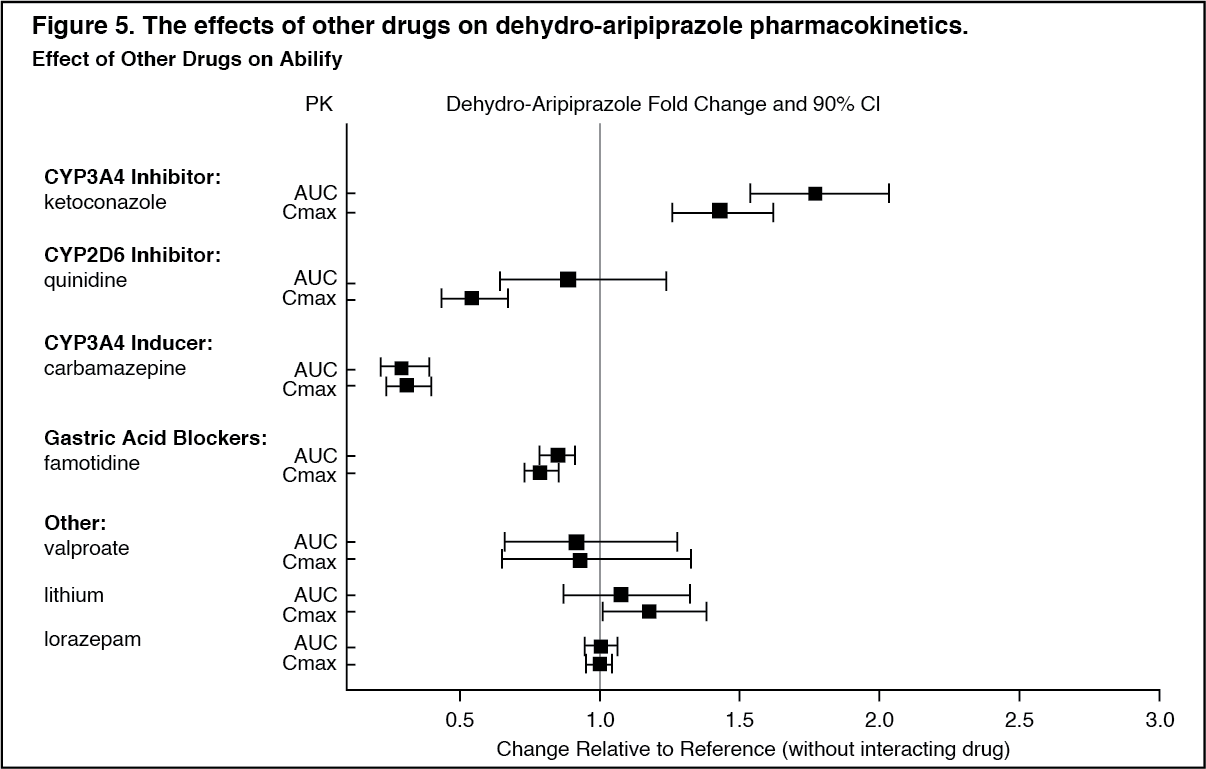 Click on icon to see table/diagram/image
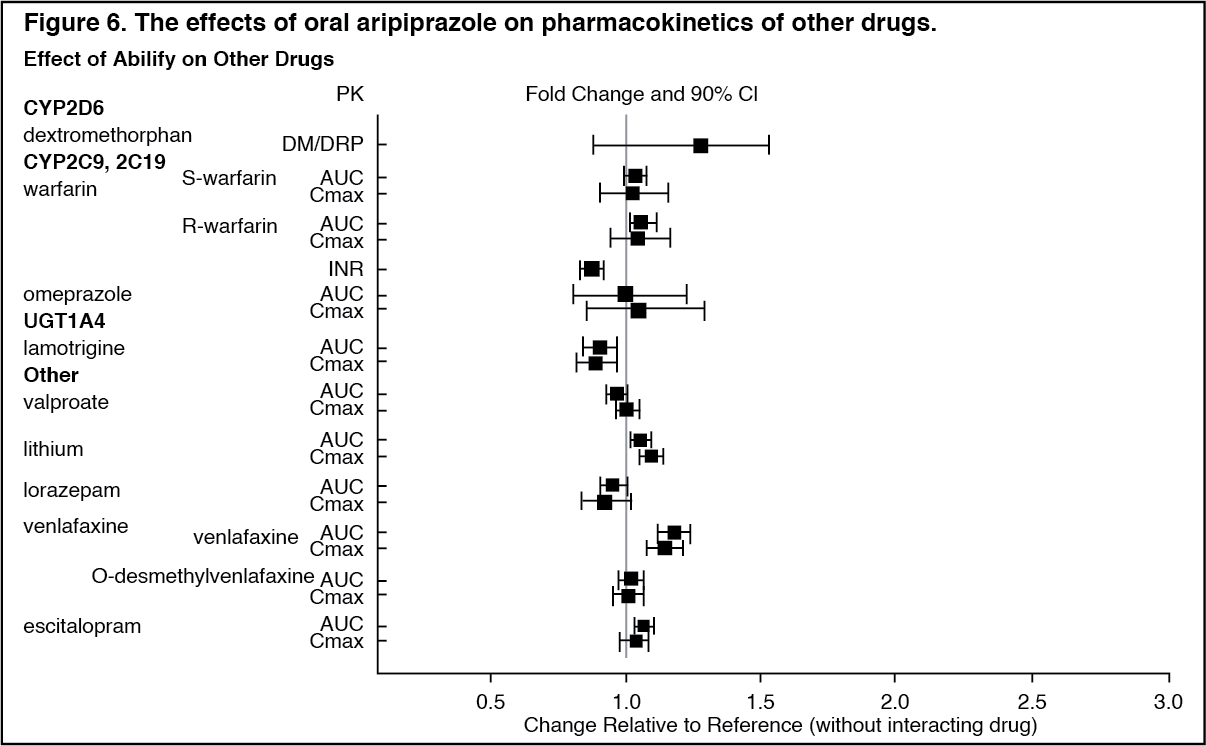
Click on icon to see table/diagram/imageThe effects of ABILIFY on the exposures of other drugs are summarized in Figure 6. A population PK analysis in patients with major depressive disorder showed no substantial change in plasma concentrations of fluoxetine (20 mg/day or 40 mg/day), paroxetine CR (37.5 mg/day or 50 mg/day), or sertraline (100 mg/day or 150 mg/day) dosed to steady-state. The steady-state plasma concentrations of fluoxetine and norfluoxetine increased by about 18% and 36%, respectively, and concentrations of paroxetine decreased by about 27%. The steady-state plasma concentrations of sertraline and desmethylsertraline were not substantially changed when these antidepressant therapies were coadministered with aripiprazole. (See Figure 6.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageStudies in Specific Populations: No specific pharmacokinetic studies have been performed with ABILIFY MAINTENA in specific populations. All the information is obtained from studies with oral aripiprazole.
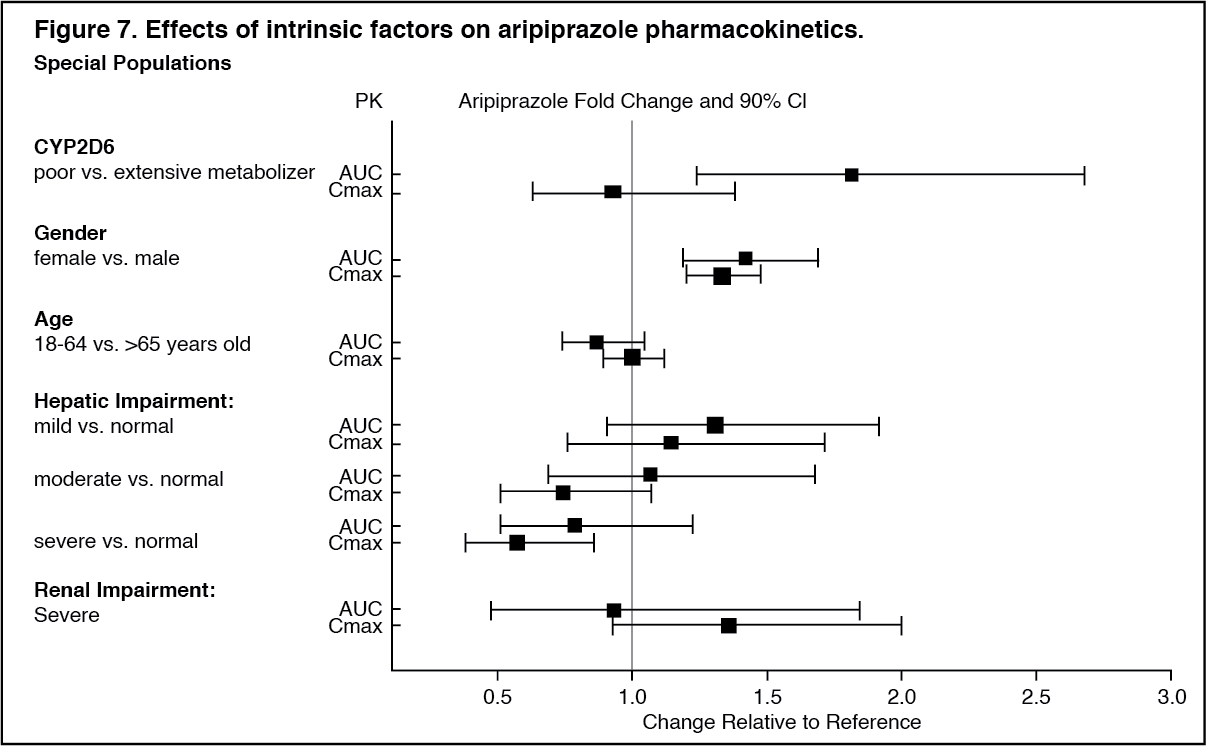
Exposures of aripiprazole and dehydro-aripiprazole in specific populations are summarized in Figure 7 and Figure 8, respectively. In addition, in pediatric patients (10 to 17 years of age) administered with oral aripiprazole (20 mg to 30 mg), the body weight corrected aripiprazole clearance was similar to the adults. (See Figures 7 and 8.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image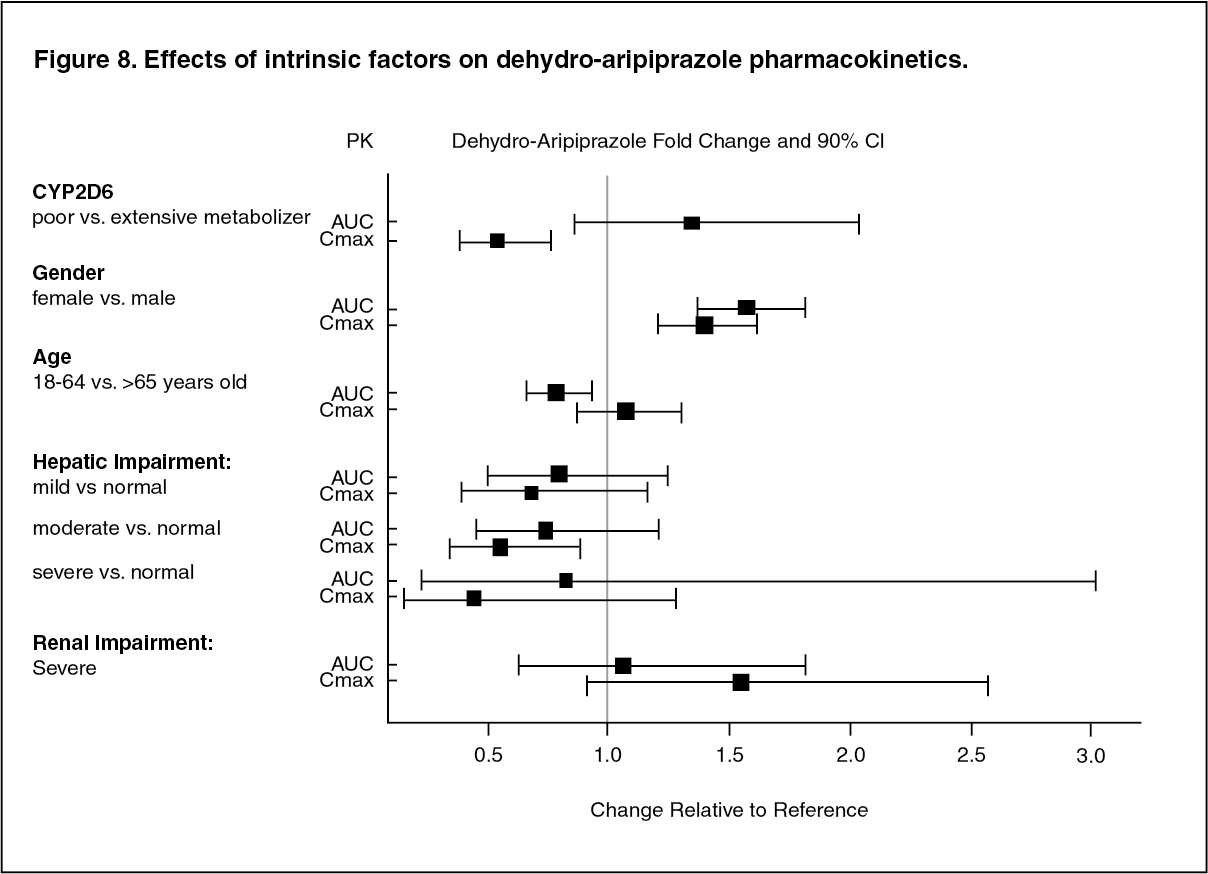 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageNONCLINICAL TOXICOLOGY: Carcinogenesis, Mutagenesis, Impairment of Fertility: Carcinogenesis: Lifetime carcinogenicity studies were conducted in ICR mice, Sprague-Dawley (SD) rats, and F344 rats. Aripiprazole was administered for 2 years in the diet at doses of 1, 3, 10, and 30 mg/kg/day to ICR mice and 1, 3, and 10 mg/kg/day to F344 rats (0.2 to 5 times and 0.3 to 3 times the maximum recommended human dose [MRHD] based on mg/m2, respectively). In addition, SD rats were dosed orally for 2 years at 10, 20, 40, and 60 mg/kg/day (3 to 19 times the MRHD based on mg/m2). Aripiprazole did not induce tumors in male mice or male rats. In female mice, the incidences of pituitary gland adenomas and mammary gland adenocarcinomas and adenoacanthomas were increased at dietary doses of 3 to 30 mg/kg/day (0.1 to 0.9 times human exposure at MRHD based on AUC and 0.5 to 5 times the MRHD based on mg/m2). In female rats, the incidence of mammary gland fibroadenomas was increased at a dietary dose of 10 mg/kg/day (0.1 times human exposure at MRHD based on AUC and 3 times the MRHD based on mg/m2); and the incidences of adrenocortical carcinomas and combined adrenocortical adenomas/carcinomas were increased at an oral dose of 60 mg/kg/day (14 times human exposure at MRHD based on AUC and 19 times the MRHD based on mg/m2).
Proliferative changes in the pituitary and mammary gland of rodents have been observed following chronic administration of other antipsychotic agents and are considered prolactin-mediated. Serum prolactin was not measured in the aripiprazole carcinogenicity studies. However, increases in serum prolactin levels were observed in female mice in a 13-week dietary study at the doses associated with mammary gland and pituitary tumors. Serum prolactin was not increased in female rats in 4-week and 13-week dietary studies at the dose associated with mammary gland tumors. The relevance for human risk of the findings of prolactin-mediated endocrine tumors in rodents is unknown.
Mutagenesis: The mutagenic potential of aripiprazole was tested in the in vitro bacterial reverse-mutation assay, the in vitro bacterial DNA repair assay, the in vitro forward gene mutation assay in mouse lymphoma cells, the in vitro chromosomal aberration assay in Chinese hamster lung (CHL) cells, the in vivo micronucleus assay in mice, and the unscheduled DNA synthesis assay in rats. Aripiprazole and a metabolite (2,3-DCPP) were clastogenic in the in vitro chromosomal aberration assay in CHL cells with and without metabolic activation. The metabolite, 2,3-DCPP, produced increases in numerical aberrations in the in vitro assay in CHL cells in the absence of metabolic activation. A positive response was obtained in the in vivo micronucleus assay in mice; however, the response was due to a mechanism not considered relevant to humans.
Impairment of Fertility: Female rats were treated with oral doses of 2, 6, and 20 mg/kg/day (0.6, 2, and 6 times the MRHD on a mg/m2 basis) of aripiprazole from 2 weeks prior to mating through day 7 of gestation. Estrus cycle irregularities and increased corpora lutea were seen at all doses, but no impairment of fertility was seen. Increased pre-implantation loss was seen at 6 and 20 mg/kg/day and decreased fetal weight was seen at 20 mg/kg/day.
Male rats were treated with oral doses of 20, 40, and 60 mg/kg/day (6, 13, and 19 times the MRHD on a mg/m2 basis) of aripiprazole from 9 weeks prior to mating through mating. Disturbances in spermatogenesis were seen at 60 mg/kg and prostate atrophy was seen at 40 and 60 mg/kg, but no impairment of fertility was seen.
Animal Toxicology and/or Pharmacology: Oral Aripiprazole: Aripiprazole produced retinal degeneration in albino rats in a 26-week chronic toxicity study at a dose of 60 mg/kg and in a 2-year carcinogenicity study at doses of 40 and 60 mg/kg. The 40 and 60 mg/kg/day doses are 13 and 19 times the MRHD based on mg/m2 and 7 to 14 times human exposure at MRHD based on AUC. Evaluation of the retinas of albino mice and of monkeys did not reveal evidence of retinal degeneration. Additional studies to further evaluate the mechanism have not been performed. The relevance of this finding to human risk is unknown.
Intramuscular Aripiprazole: The toxicological profile for aripiprazole administered to experimental animals by intramuscular injection is generally similar to that seen following oral administration at comparable plasma levels of the drug. With intramuscular injection, however, injection-site tissue reactions are observed that consist of localized inflammation, swelling, scabbing and foreign-body reactions to deposited drug. These effects gradually resolved with discontinuation of dosing.
After 26 weeks of treatment in rats, the no-observed-adverse-effect level (NOAEL) was 50 mg/kg in male rats and 100 mg/kg in female rats, which are approximately 1 and 2 times, respectively, the maximum recommended human 400 mg dose of aripiprazole extended-release injectable suspension on a mg/m2 body surface area. At the NOAEL in rats, the AUC7d values were 14.4 μg∙h/mL in males and 104.1 μg∙h/mL in females. In dogs at 52 weeks of treatment at the NOAEL of 40 mg/kg, which is approximately 3 times the MRHD (400 mg) on a mg/m2 body surface area, the AUC7d values were approximately 59 μg∙h/mL in males and 44 μg∙h/mL in females. In patients at the MRHD of 400 mg, the AUCτ (0-28 days) was 163 μg∙h/mL. For comparison to this human AUC, extrapolating the animal AUC7d values to an AUC28d results in AUC28d values of approximately 58 and 416 μg∙h/mL for male and female rats, respectively, and 236 and 175 μg∙h/mL for male and female dogs, respectively.